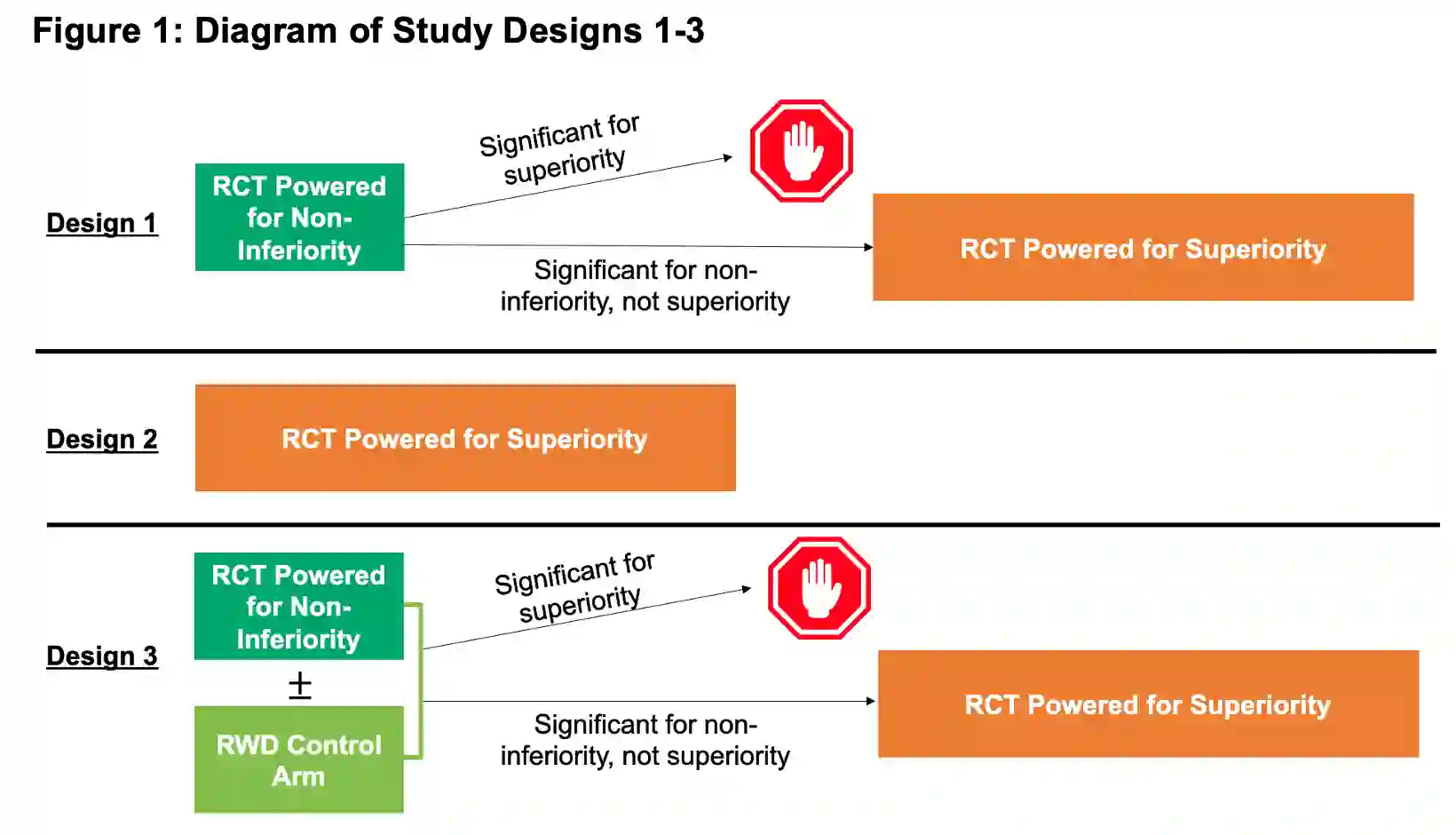
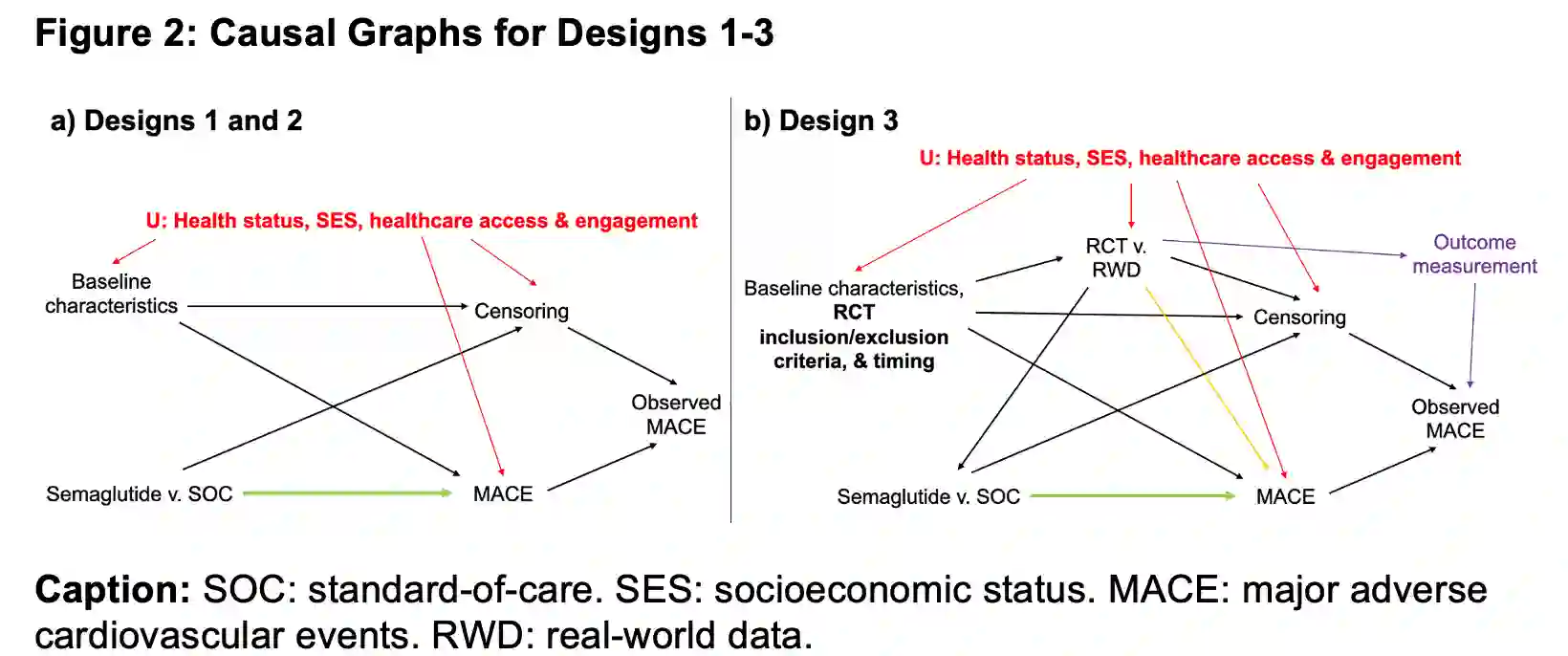
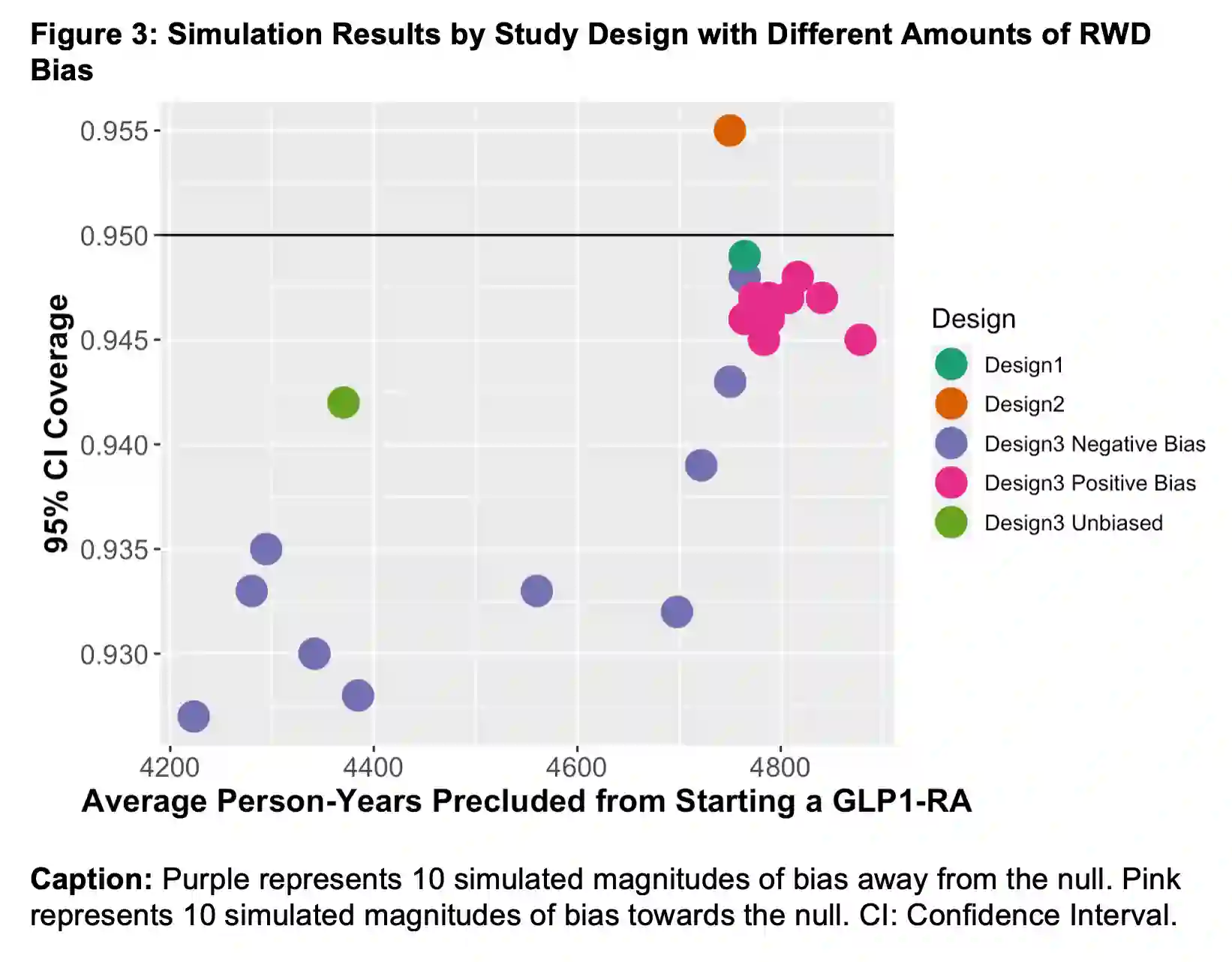
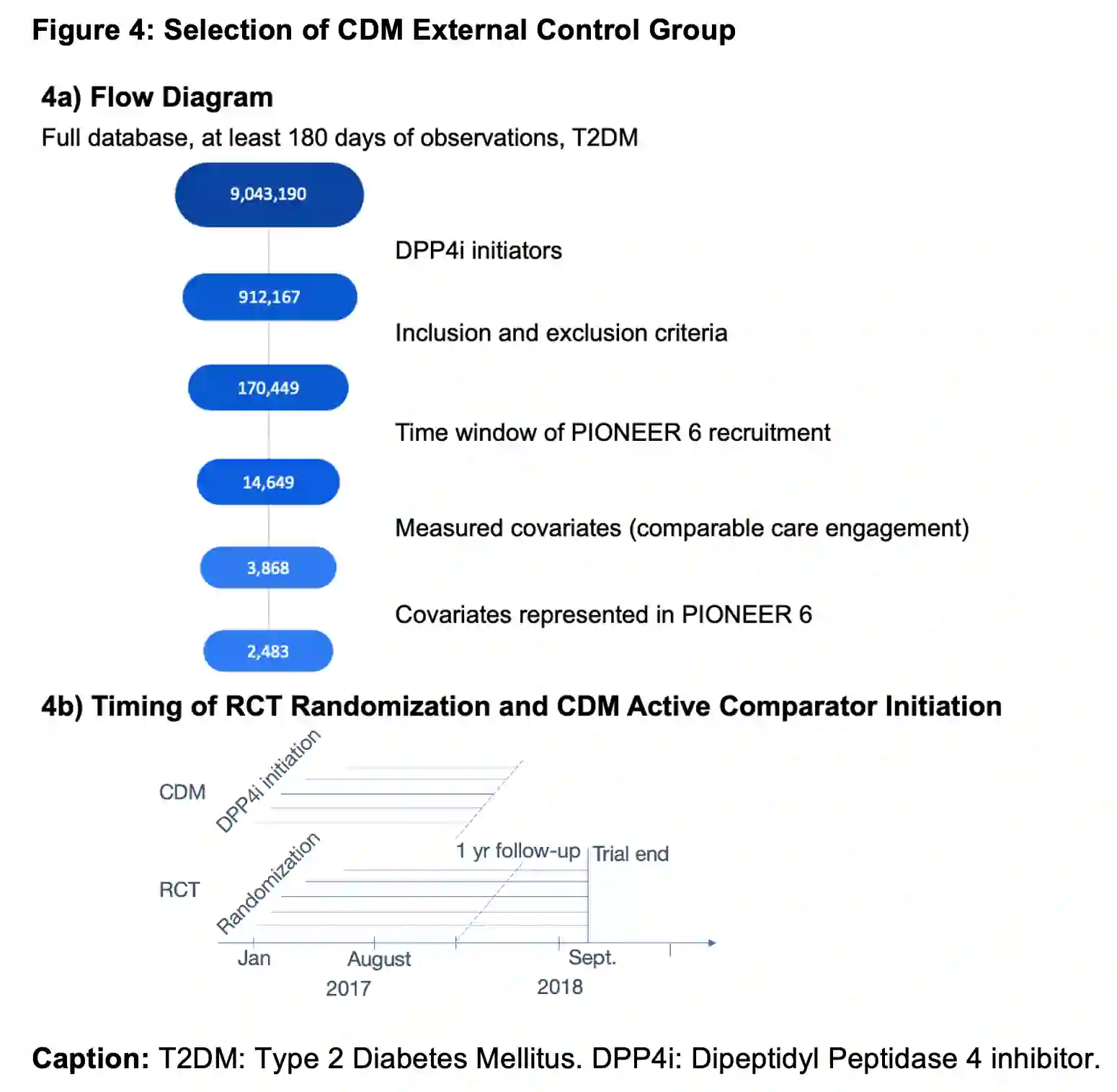
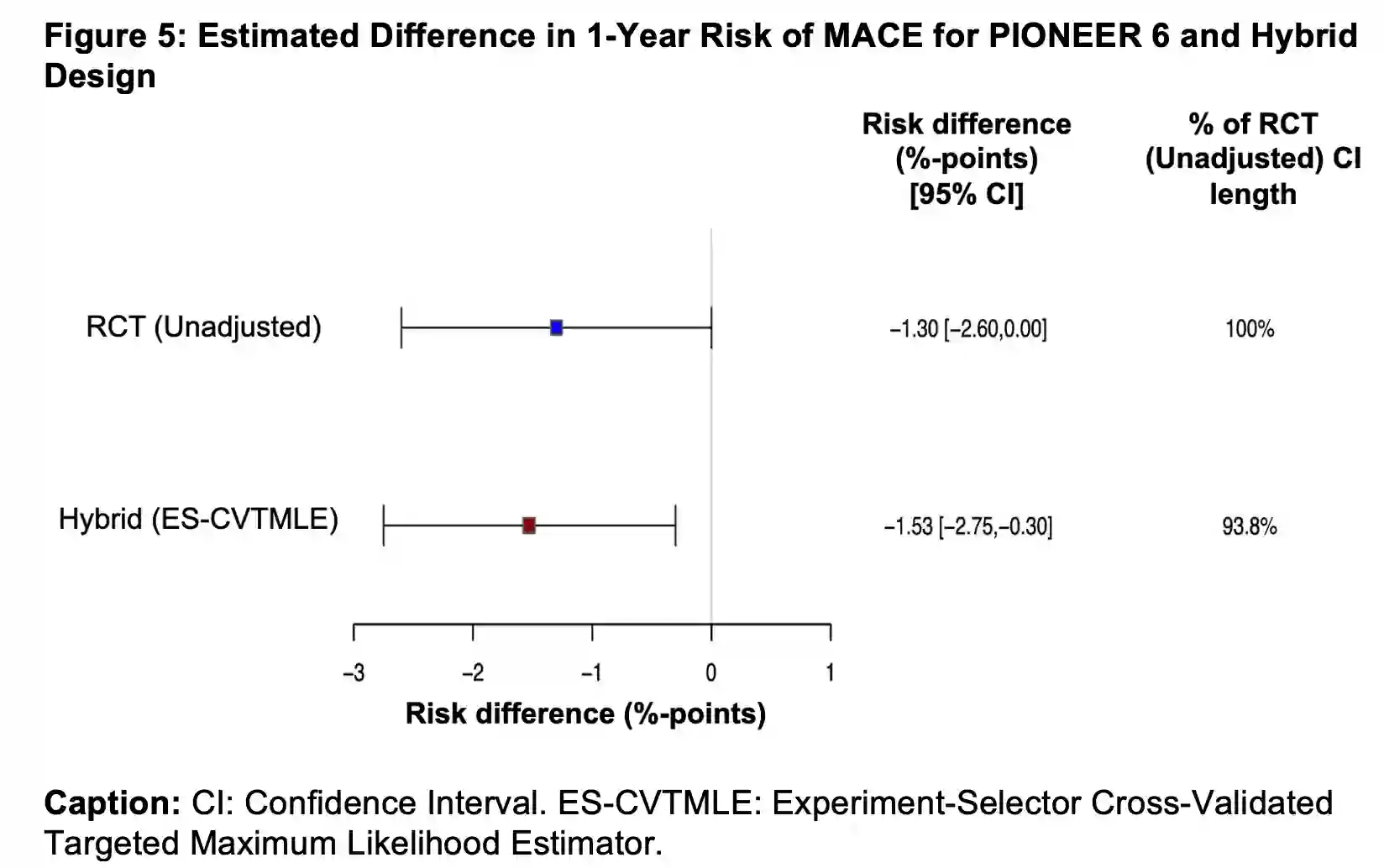
Introduction: Increasing interest in real-world evidence has fueled the development of study designs incorporating real-world data (RWD). Using the Causal Roadmap, we specify three designs to evaluate the difference in risk of major adverse cardiovascular events (MACE) with oral semaglutide versus standard-of-care: 1) the actual sequence of non-inferiority and superiority randomized controlled trials (RCTs), 2) a single RCT, and 3) a hybrid randomized-external data study. Methods: The hybrid design considers integration of the PIONEER 6 RCT with RWD controls using the experiment-selector cross-validated targeted maximum likelihood estimator. We evaluate 95% confidence interval coverage, power, and average patient-time during which participants would be precluded from receiving a glucagon-like peptide-1 receptor agonist (GLP1-RA) for each design using simulations. Finally, we estimate the effect of oral semaglutide on MACE for the hybrid PIONEER 6-RWD analysis. Results: In simulations, Designs 1 and 2 performed similarly. The tradeoff between decreased coverage and patient-time without the possibility of a GLP1-RA for Designs 1 and 3 depended on the simulated bias. In real data analysis using Design 3, external controls were integrated in 84% of cross-validation folds, resulting in an estimated risk difference of -1.53%-points (95% CI -2.75%-points to -0.30%-points). Conclusions: The Causal Roadmap helps investigators to minimize potential bias in studies using RWD and to quantify tradeoffs between study designs. The simulation results help to interpret the level of evidence provided by the real data analysis in support of the superiority of oral semaglutide versus standard-of-care for cardiovascular risk reduction.
翻译:引言:对真实世界证据日益增长的兴趣推动了纳入真实世界数据(RWD)的研究设计发展。基于因果路线图,我们提出了三种设计来评估口服司美格鲁肽与标准治疗相比在主要不良心血管事件(MACE)风险方面的差异:1)实际序列的非劣效性和优效性随机对照试验(RCTs),2)单一RCT,以及3)混合随机化-外部数据研究。方法:混合设计考虑将PIONEER 6 RCT与RWD对照组整合,采用实验选择器交叉验证目标最大似然估计量。通过模拟,我们评估了每种设计的95%置信区间覆盖率、统计功效以及参与者被禁止接受胰高血糖素样肽-1受体激动剂(GLP1-RA)的平均患者时间。最后,我们估计了混合PIONEER 6-RWD分析中口服司美格鲁肽对MACE的影响。结果:在模拟中,设计1和设计2的表现相似。设计1和设计3在覆盖率降低与无GLP1-RA可能性的患者时间之间的权衡取决于模拟的偏倚。在使用设计3的真实数据分析中,外部对照在84%的交叉验证折中被整合,估计风险差异为-1.53个百分点(95%置信区间:-2.75至-0.30个百分点)。结论:因果路线图有助于研究者最小化使用RWD的研究中潜在偏倚,并量化研究设计之间的权衡。模拟结果有助于解释真实数据分析提供的证据水平,以支持口服司美格鲁肽在降低心血管风险方面优于标准治疗。